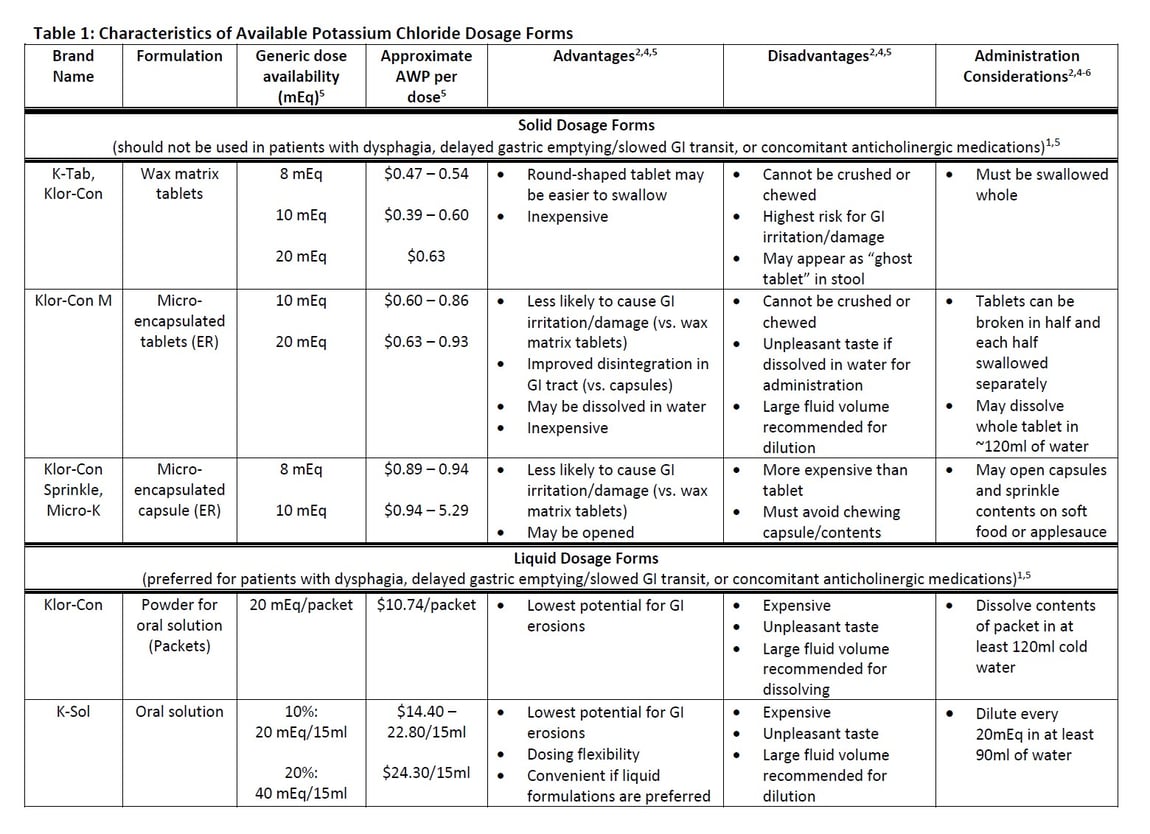
Diuretics can be especially useful to the hospice clinician for managing fluid retention or edema that commonly occurs in patients with heart failure, cirrhosis, and cancer. Unfortunately, long-term use of loop and thiazide diuretics can lead to hypokalemia, which can be particularly challenging to treat in patients with dysphagia given the fact that many potassium chloride (KCl) supplements are inherently large and difficult to swallow. It’s important to consider the potential alternatives for patients with dysphagia and the advantages and disadvantages of the various KCl formulations that are currently available: tablets, capsules, powder for solution, and oral solution (Table 1). When choosing a KCl product, the hospice team should consider special instructions for administration, palatability, risk for adverse effects, and contraindications of each.
Gastrointestinal (GI) irritation and damage are well-known side effects of KCl supplements. This can be especially concerning in patients with dysphagia and patients who spend much of their time lying down since KCl tablets can get stuck in the esophagus and potentially cause damage due to prolonged contact with the mucosa.1.2 Interestingly, esophageal injury related to KCl use can lead to dysphagia – patients don’t always experience pain so the damage could go unnoticed until fibrotic strictures that narrow the esophageal opening develop.3
Solid dosage forms are more likely to cause GI irritation than liquid dosage forms. Among the different solid forms, the risk is lower with capsules and microencapsulated tablets compared to wax matrix tablets.4 Although the oral solution is a safer alternative, cases of esophagitis have still been reported with this formulation. As a result, all KCl products should be used cautiously in patients with dysphagia or those that spend significant time in the recumbent position. Patients should be instructed to report any symptoms of drug-induced esophagitis including the feeling like a pill is stuck in the throat, burning, and retrosternal pain.1
Drug-interaction programs in Lexi-Comp, Facts & Comparisons, Micromedex, and Epocrates all flag the use of solid oral dosage forms of KCl with anticholinergic medications as a contraindicated drug combination. While there isn’t consistent or robust data to support it, clinicians should consider the risk for GI irritation when KCl supplements are combined with anticholinergic medications due to their tendency to slow gastric motility and maintain prolonged contact with gastric and esophageal mucosa.1In the event that a patient requires continued therapy with anticholinergic medications, liquid KCl formulations should be used preferentially over tablets and capsules. For the same reason, liquid formulations might also be preferred in patients with conditions causing delayed gastric emptying such as diabetes, Parkinson Disease, multiple sclerosis, or hypothyroidism.
To reduce the risk for GI-related adverse effects, patients should be advised to follow their KCl doses with plenty of water (at least 100mL) and to stay in an upright position for 5-10 minutes immediately following administration. For bedbound patients, consider elevating the head of the bed for patients who have difficulty sitting up for prolonged periods.1 The product labeling for all KCl products states that they should be taken with food and water or other liquid and the prescribing information for the oral solution indicates that every 20mEq should be diluted in at least 90mL (3 oz.) of water to minimize to minimize GI irritation and discomfort.5,6 In other words, ordering KCl oral solution may not be an ideal solution for a patient with increasing difficulty swallowing and trouble consuming even minimal amounts of liquids, not to mention the unpleasant, salty taste that patients report despite it being a flavored medication. And, although the microencapsulated tablets will dissolve in much less than the 4 ounces of water recommended in the product labeling, administering a more concentrated product could potentially increase the risk for GI damage.
The challenges of drug administration in patients approaching end-of-life as well as the risks for KCl-related drug interactions and adverse effects underline the importance of deprescribing anticholinergic medications and re-evaluating the need for continued supplementation on an ongoing basis.
Reviewed by: Melissa Corak, PharmD, Clinical Pharmacist, OnePoint Patient Care
References:
- Zarowitz, BJ. Oral solid potassium chloride and anticholinergic medications: A new drug interaction for an old drug? Geriatric Nursing. 2006;27(6):329-333.
- Pl Detail-Document, Potassium and anticholinergic drug interaction. Pharmacist’s Letter/Prescriber’s Letter. October 2011.
- Jaspersen, D. Drug-induced oesophageal disorders: pathogenesis incidence, prevention and management. Drug Safety. 2000;22:237-249.
- PL Detail-Document, Comparison of potassium salts. Pharmacist’s Letter/Prescriber’s Letter. April 2016.
- Lexicomp Online, Lexi-Drugs, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc; 2019; Accessed May 30, 2019.
- Potassium chloride solution [package insert]. Levittown, PA. Bio-Pharm, Inc; 2014.