Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used to treat pain and inflammation.1,2With more than 20 different (but similarly effective) NSAIDs on the market, why would a provider prescribe or recommend one NSAID over another?3-5
Cox-Selectivity
NSAIDs inhibit cyclooxygenase (COX) enzymes to prevent the production of prostaglandins, which are chemical mediators of pain and inflammation.1-6 There are relevant COX enzymes; COX-1 and COX-2. COX-1 is present in most tissues and plays a role in normal cellular processes.1-4,6 COX-2 produces pro-inflammatory prostaglandins and is expressed during periods of inflammation.2,6,7 Different NSAIDs inhibit COX to varying degrees and this influences their side effect profiles.5 You can read more about COX enzymes and the significance of COX-selectivity here.
Side effects
NSAIDs have known adverse effects including gastrointestinal (GI) ulceration and bleeding, hypertension, edema, heart attack, stroke, and heart failure.1,7 NSAIDs with greater selectivity for COX-2 (e.g., celecoxib) are typically regarded as having lower GI risk, but higher cardiovascular (CV) risk.6,7Renal adverse effects including electrolyte imbalance, reduced GFR, and CKD might also occur, though these are less common and more likely to arise when higher doses are used for longer durations.1,5 NSAIDs should be carefully chosen with consideration for patient-specific risk factors (Table 1) to minimize the risk of exacerbating GI or cardiovascular disease (Table 2).
Table 1 – Risk Factors for NSAID Related Adverse Events7
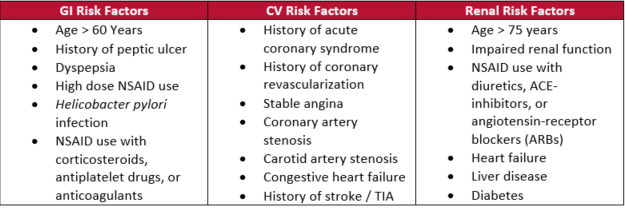
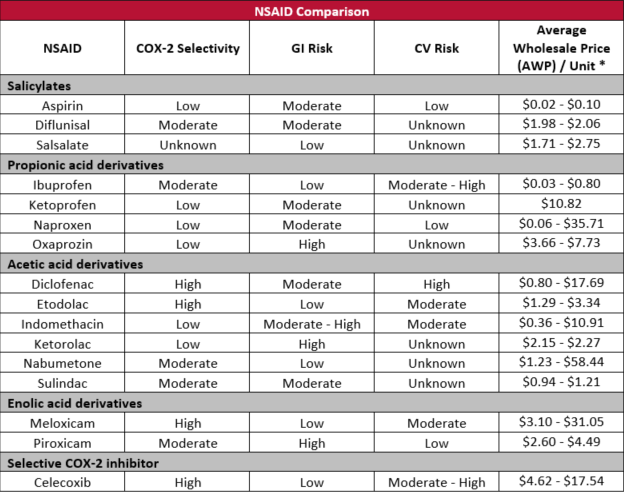
Table 2. – NSAID Comparison: COX-2 Selectivity, GI/CV Risk, and Cost4,6-9
GI: gastrointestinal; CV: cardiovascular
*Oral dosage forms only; Unit = tablet, capsule, milliliter
Other considerations
It’s hard to ignore that some NSAIDs cost more than others, but sometimes more money may get you more favorable safety and tolerability profiles (Table 2). For example, celecoxib may be more expensive than other NSAIDs, but it’s selective for COX-2 and is associated with a lower risk of GI adverse events.6 Also, some NSAIDs might be more advantageous than others based on dosage form availability. For example, diclofenac is commercially available in topical preparations. Despite sharing the same warnings as other systemic NSAIDs, topical diclofenac might be a reasonable choice for patients with localized pain and GI or CV risk factors, since very little is absorbed systemically (about 95% less systemic exposure than with oral administration) and it appears to have a safety profile comparable to placebo.6 In other cases, therapy selection might be driven by clinician preference and familiarity, or indication-specific evidence for certain NSAIDs. Read more about choosing NSAID therapy here.
Written by:
John Corrigan, PharmD
Clinical Pharmacist, OnePoint Patient Care
John’s primary responsibilities as a clinical pharmacist at OnePoint Patient Care are staff and partner education, medication utilization reviews, and assisting with formulary development and maintenance. He attended the University of Iowa for both undergraduate studies and pharmacy school. He earned a PharmD from the University of Iowa College of Pharmacy in 2013. He was first introduced to hospice and OnePoint Patient Care as a 4th year pharmacy student, completing a 5-week elective clinical hospice pharmacy rotation. He started his employment with OnePoint Patient Care as a staff pharmacist in 2014. He transitioned to his current role, as a clinical pharmacist, in the spring of 2019.
References
- Wongrakpanich S, Wongrakpanic A, Melhado K, Rangaswami J. A Comprehensive Review of Non-Steroidal Anti-Inflammatory Drug Use in The Elderly. Aging and Disease. 2018;9(1):143-150. Doi:14336/AD.2017.0306
- Gorczyca P, Manniello M, Pisano M, Avena-Woods C. NSAIDs: Balancing the Risks and Benefits. US Pharm. 2016;41(3):24-26. https://www.uspharmacist.com/article/nsaids-balancing-the-risks-and-benefits
- Solomon D. NSAIDs: Pharmacology and mechanism of action. UpToDate. Updated July 30, 2021. Accessed April 28, 2022. https://www.uptodate.com/contents/nsaids-pharmacology-and-mechanism-of-action
- Patrono C, Baigent C. Nonsteroidal Anti-Inflammatory Drugs and the Heart. Circulation. 2014;129:907-916. Doi: 1161/CirculationAHA.113.004480
- Ho K Y, Cardosa M, Chaiamnuay S, et al. Practice Advisory on the Appropriate Use of NSAIDs in Primary Care. Journal of Pain Research. 2020;13:1925-1939. Doi:2147/JPR.S247781
- Managing NSAID Risks. Pharmacist’s Letter. July 2018. Accessed April 29, 2022. https://pharmacist.therapeuticresearch.com/Content/Segments/PRL/2017/Jan/Managing-NSAID-Risks-10557
- Safety Comparison of NSAIDs. Pharmacist’s Letter / Prescriber’s Letter. January 2017. Accessed May 23, 2022. https://pharmacist.therapeuticresearch.com/en/Content/Segments/PRL/2017/Jan/Safety-Comparison-of-NSAIDs-10556
- Accessed May 25, 2022.
- Scarpignato C, Lanas A, Blandizzi C, et al. Safe Prescribing of Non-steroidal Anti-inflammatory Drugs in Patients with Osteoarthritis – An Expert Consensus Addressing Benefits as well as Gastrointestinal and Cardiovascular Risks. BMC Medicine. 2015;13(55):1-22. Doi:1186/s12916-015-0285-8
- Ju Z, et al. Recent development on COX-2 inhibitors as promising anti-inflammatory agents: The past 10 years. Acta Pharmaceutica Sinica B. 2022;12(6):2790-2807. Doi:1016/j.apsb.2022.01.002